By Dr Catherine W. Dunne, MSc.D., RGN (GPN), M.H.I.T. Holistic Healthcare Wexford
There’s a short window in spring when stinging nettle is at its best.
The young shoots are tender, vibrant, and full of life. They haven’t toughened yet, and interestingly, they’re far less “stingy” to handle when picked correctly.
This is when nettle shifts from being a nuisance in the garden… to one of the most useful plants you can bring into your daily routine.
Why Spring Nettles Are Different
Young nettle leaves are rich in:
Natural enzymes
Vitamin C
Iron
Magnesium
Calcium
Chlorophyll
Plant compounds that help reduce oxidative stress
At this stage, the plant is in active growth. Everything is moving, building, and regenerating.
And that’s exactly what it offers the body.
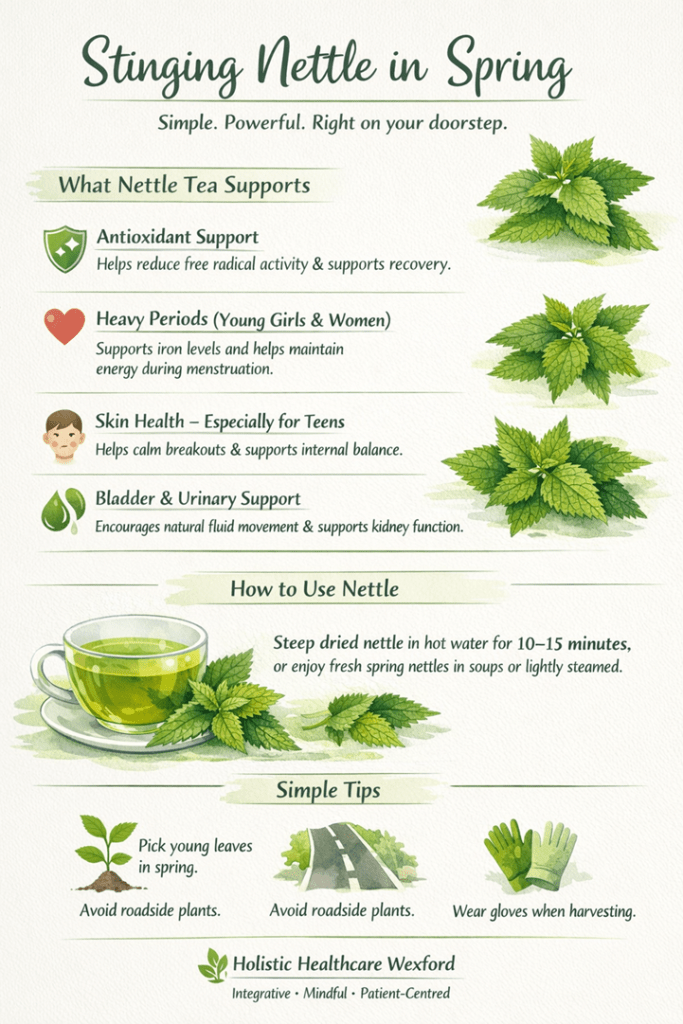
WHAT NETTLE TEA SUPPORTS
A simple cup of nettle tea, taken regularly, can do far more than most people expect. It works quietly in the background, supporting the body where it needs it most.
Antioxidant support
Nettle helps reduce free radical activity in the body.
This matters more than people realise. Oxidative stress is linked to fatigue, inflammation, skin issues, and slower recovery.
A daily nettle tea is a quiet way of supporting the body at that level.
Support for heavy periods (young girls & women)
This is one of the old uses and still one of the most relevant.
Nettle:
Supports iron levels
Helps maintain energy
Provides minerals needed during blood loss
Nettle provides natural support for iron levels, helping maintain energy during heavier menstrual cycles. It also supplies key minerals the body draws on during blood loss.
Taken as a tea, it offers gentle support without complication.
Skin support – especially teenagers
When skin is flaring, spots, congestion, breakouts, the body is often:
Under pressure
Slightly inflamed
Not clearing waste efficiently
The body often reflects internal imbalance rather than just surface issues.
Nettle supports the body by helping reduce inflammatory load, improving nutrient availability, and encouraging natural internal “clearing.”
It’s not a quick fix, but taken daily and over time, it brings a steadiness the skin responds well in a noticeable way, too.
Bladder and urinary support
Even as a simple tea, nettle supports normal kidney and urinary function.
It gently encourages fluid movement through the body without being harsh or depleting. This makes it particularly useful when the system feels sluggish or under strain.
It’s not harsh. It doesn’t deplete.
It supports the body in doing what it’s meant to do anyway.
How to Use It
Nettle doesn’t need complicated preparation. In fact, its strength lies in its simplicity.
A teaspoon or two of dried nettle steeped in hot water for 10–15 minutes is enough to create a mineral-rich infusion.
Taken once or twice daily, it becomes a steady support rather than a quick intervention.
Fresh young nettle in spring can also be used in soups or lightly steamed, offering the same benefits in a more food-based form.
With nettle, consistency matters far more than quantity.
RECAP:
✔️ Fresh nettle (spring)
Pick young tops (gloves recommended)
Use in soups, broths, or lightly steamed
Can also be used fresh for tea
✔️ Tea
1–2 teaspoons dried nettle per cup
Steep 10–15 minutes
Drink 1–3 cups daily
Consistency matters more than quantity.
A few practical notes
Avoid picking near roadsides or sprayed areas
If on diuretics or blood pressure medication, just be mindful
Pick young leaves in spring, when the plant is at its most vibrant
Avoid roadside or sprayed areas
Use gloves when harvesting fresh nettle
In most cases, nettle as a tea is safe and well tolerated
Final Thought
Nettle isn’t exotic. It’s not expensive. It doesn’t come in a glossy package.
And yet, every spring, it shows up offering exactly what the body often needs:
👉 nourishment 👉 support 👉 balance
Sometimes the simplest plants are the ones worth paying attention to.
I hope you feel inspired. Look after your body, and it will keep you healthy.
Dr Catherine W. Dunne is a Registered General Nurse with over 37 years of clinical experience in primary care in Ireland. Alongside her work in General Practice Nursing, she is the founder of Holistic Healthcare Wexford and co-founder of Aumvedas Academy.
With a background that bridges conventional medicine and holistic practice, Catherine has a particular interest in the area where patients are often told “everything is normal,” yet still feel unwell. Her work focuses on helping people understand what their body is communicating, especially in relation to energy, stress, metabolic function, and recovery.
Through a combination of clinical knowledge and holistic support, she works with individuals to restore balance, improve resilience, and support long-term wellbeing.
Based in Wexford, Ireland.
Disclaimer The information provided in this article is for general educational purposes only and is not intended as medical advice, diagnosis, or treatment. While every effort is made to ensure accuracy, individual health needs can vary. Always consult your GP or a qualified healthcare professional before making changes to your health routine, especially if you have an existing condition, are taking medication, or are pregnant.
You can take Vitamin D, Magnesium, and Calcium—and still not get the results you expect. Sometimes, the missing piece is not what you take, but what helps your body use it.
By Dr Catherine W. Dunne, MSc.D., RGN (GPN) Holistic Healthcare Wexford
Boron is one of those nutrients.
It may only be required in trace amounts, but its impact on bone health, hormones, inflammation, and Vitamin D function makes it a valuable addition to a well-structured health plan.
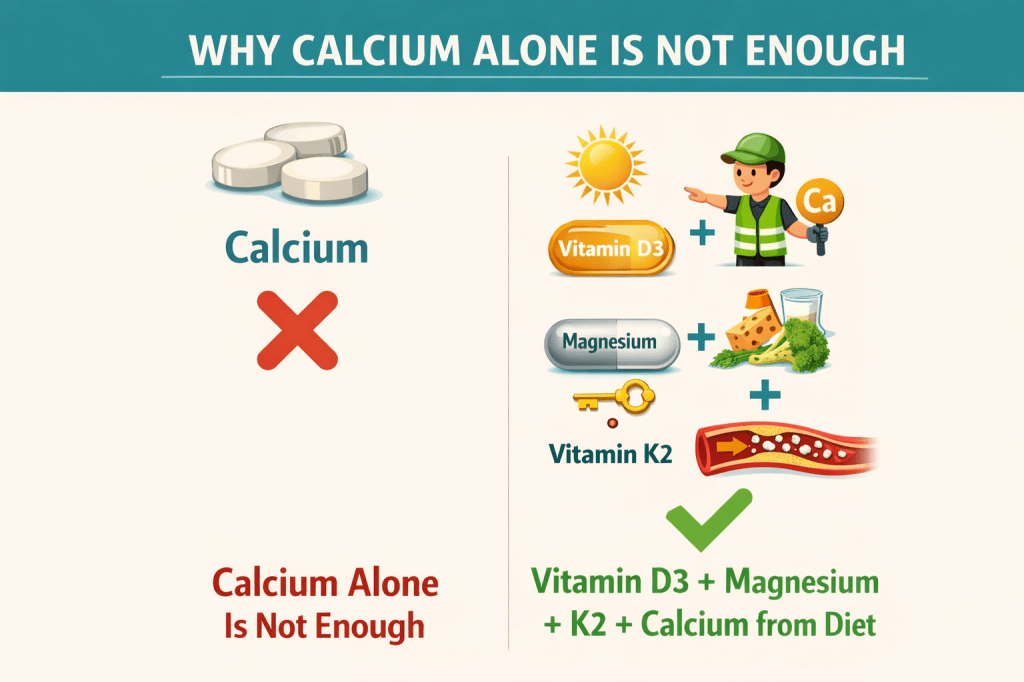
Bone Health: More Than Just Calcium
When it comes to bones, most people think of Calcium. But Calcium alone is only part of the picture.
Boron helps the body to improve Calcium retention, enhance Magnesium utilisation, and support Vitamin D activation. This creates a more efficient system for maintaining bone density and strength.
Emerging research also suggests Boron may help reduce joint discomfort and stiffness, particularly in osteoarthritis, by supporting a balanced inflammatory response.
In clinical practice, this is often seen in patients whose bone markers or symptoms do not improve despite adequate Calcium and Vitamin D intake.
A Natural Anti-Inflammatory Support
Chronic, low-grade inflammation is at the root of many modern health concerns.
Boron has been shown to reduce inflammatory markers such as CRP, modulate immune responses, and support tissue recovery.
This makes it a useful addition in cases of joint pain, post-viral fatigue, and general inflammatory states.
In clinical settings, this may be relevant in patients presenting with persistent low-grade inflammatory symptoms.
Hormonal Balance: A Quiet Regulator
One of Boron’s most interesting roles is its influence on hormones.
It has been shown to influence free testosterone levels, support healthy oestrogen metabolism, and reduce sex hormone binding globulin (SHBG).
This means more hormones are available in their active form, which may benefit perimenopause, menopause, and low energy states.
Boron and Vitamin D: A Powerful Partnership
Boron plays a supportive role in how the body uses Vitamin D.
It helps extend the half-life of Vitamin D, improve Magnesium efficiency, and support proper Calcium direction alongside Vitamin K2.
Together, Vitamin D, Magnesium, Vitamin K2, and Boron create a more balanced and effective system.
Boron may also play a supportive role in thyroid function through its interaction with mineral balance and hormone regulation.
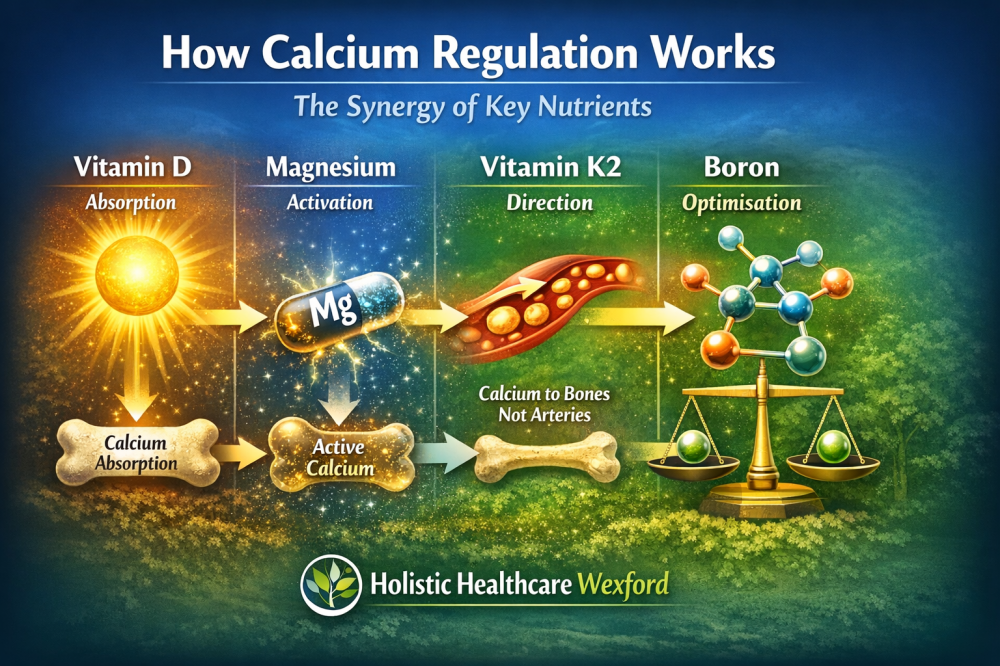
This is how these nutrients work together in the body:
Cognitive and Nervous System Support
Low Boron intake has been associated with reduced concentration, slower cognitive processing, and brain fog.
Adequate levels may support mental clarity and neurological function.
Dietary Sources of Boron
Boron is found naturally in avocados, raisins, prunes, nuts (especially almonds), and leafy green vegetables.
However, modern diets often provide lower than optimal intake.
Supplementation
Typical intake ranges from 3 mg daily for general support, with 6 mg often used in short-term therapeutic protocols.
There is rarely a need to exceed this range.
Safety Considerations
Avoid high doses in pregnancy and use caution in kidney disease. As with all nutrients, balance is key.
Clinical Perspective
Boron is often the missing link in protocols where bone support, Vitamin D response, hormonal balance, or inflammation management are not progressing as expected.
Final Thoughts
Boron helps the body use what is already there more efficiently. In many cases, health does not improve because something is missing but because what is already there is not being used properly.
Boron does not replace your core nutrients, it helps them work properly.
I hope you feel inspired. Look after your body, and it will keep you healthy.
Catherine
CWD 27 March 2026/Ireland
About the Author
Dr Catherine W. Dunne MSc.D., RGN, M.H.I.T. is a nurse, holistic practitioner, and educator based in Wexford, Ireland. With over 35 years of experience in healthcare and energy-based healing modalities, she integrates conventional medical knowledge with holistic approaches to support whole-person well-being.
Catherine is the founder of Holistic HealthCare Wexford and co-founder of Aumvedas Academy, where she teaches courses in holistic health, energy medicine, and integrative healing practices.
Her work focuses on empowering people to understand the body as an intelligent system capable of healing when supported with the right knowledge, nutrition, and energetic balance.
Learn more: Holistic HealthCare Wexford Aumvedas Academy
Disclaimer
The information provided in this article is for educational purposes only and is not intended as medical advice. Always consult a qualified healthcare professional before starting any new supplement or health intervention.
Before assuming something complex is wrong, it is always wise to make sure the body has the nutrients it quietly depends on every day.
Dr Catherine W. Dunne MSc.D., RGN Holistic HealthCare Wexford & Aumvedas Academy Nurse, Medical Intuitive and Holistic Practitioner
They do not arrive with much fanfare. They are not advertised everywhere. And yet, when they begin to run low, the body starts sending little signals that something is not quite right.
Zinc is one of those nutrients.
It plays a role in hundreds of processes throughout the body — immunity, digestion, hormone balance, brain chemistry, sleep regulation, wound healing, and how well we cope with stress.
In practice, I often see people struggling with a collection of symptoms rather than a single complaint. Poor sleep, frequent infections, low resilience to stress, digestive discomfort, brain fog, or stubborn fatigue.
Sometimes the missing piece is not complicated at all. Sometimes it is simply that the body has run a little short of the minerals it depends on every day. And zinc is one of the most important of those.
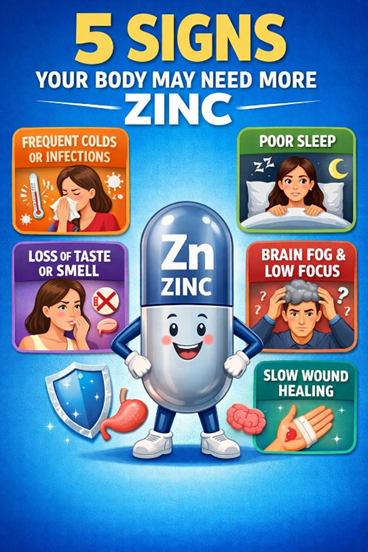
Here are five early signs your body may be asking for more zinc:
Why zinc matters so much
Zinc is involved in more than 300 enzyme reactions in the body and influences thousands of cellular processes.
It supports:
immune defence
wound healing
skin repair
hormone production
pancreatic function
neurotransmitter balance
cognitive performance
antioxidant protection
tissue growth and repair
It also plays an important role in the brain, thymus gland, digestive system, and stress response.
In other words, zinc is deeply woven into how the body maintains balance.
Early signs zinc may be running low
Zinc deficiency rarely announces itself dramatically in the beginning. Instead, it tends to show up as small persistent changes that people often dismiss.
Some early clues may include:
reduced taste or smell
poor appetite
bloating or digestive discomfort
slow wound healing
frequent colds or infections
white spots on fingernails
thinning hair
low mood
poor sleep
reduced stress tolerance
None of these symptoms alone proves a deficiency, of course. But when several appear together, it is often worth taking a closer look at nutritional foundations.
Zinc, stress and the cortisol connection
Modern life places the body under considerable stress — emotional stress, work stress, sleep disruption, inflammation, infections, and environmental factors.
One of the body’s main stress hormones is cortisol.
In short bursts, cortisol is helpful. It allows us to respond quickly and manage challenges. But when stress becomes chronic, cortisol can begin to disrupt several systems in the body.
One of the things chronic stress does is increase zinc loss.
At the same time, zinc is needed to support the immune system, regulate inflammation, and stabilise the nervous system. So when stress increases, the body may actually require more zinc, while at the same time losing more of it.
Over time this can become a loop:
stress increases cortisol ↓ cortisol contributes to zinc depletion ↓ low zinc reduces resilience ↓ fatigue and inflammation rise ↓ stress becomes harder to manage
Breaking that cycle sometimes begins with restoring the body’s basic nutritional building blocks.
Zinc and the immune system
Zinc is essential for the healthy function of the thymus gland, which sits behind the breastbone.
The thymus plays a central role in the development of T-cells, the immune cells that help recognise and fight infections.
When zinc levels fall, the thymus becomes less active and immune resilience can decline. This may partly explain why people with low zinc status sometimes notice that they seem to “catch everything” going around.
As we age, thymus activity naturally declines, which makes maintaining good zinc levels even more relevant.
Zinc and the brain
The brain contains surprisingly high concentrations of zinc.
It participates in the regulation of several neurotransmitters including:
dopamine
serotonin
GABA
glutamate
These chemical messengers influence mood, motivation, attention, memory, and sleep.
When zinc levels are suboptimal, people may notice changes such as:
brain fog
reduced concentration
lower mood
mental fatigue
disrupted sleep patterns
This is one reason zinc has attracted increasing attention in research around mood, cognitive function, and attention regulation.
A quiet conversation around attention and ADHD
Something I hear more often now in practice is adults wondering whether long-standing struggles with focus, motivation or mental organisation may be related to ADHD.
Many adults are seeking assessments for the first time in their lives.
While ADHD is a complex neurodevelopmental condition with many contributing factors, nutrition does influence brain chemistry in meaningful ways.
Zinc, for example, plays a role in dopamine metabolism, a neurotransmitter that is strongly linked with attention, reward signalling, and motivation.
Several studies have found that some children — and adults — with attention difficulties show lower zinc levels than average.
This does not mean zinc deficiency causes ADHD. Human biology is never that simple.
But it does remind us that before labelling the brain as “broken”, it is wise to make sure the body has the nutritional tools it needs to function well.
Sometimes the brain is not faulty. Sometimes it is simply under-supported.
What if you do not eat shellfish or red meat?
Oysters and shellfish are among the richest sources of zinc in the human diet. Red meat is another significant contributor.
If these foods are not eaten, zinc intake can become marginal over time, especially if the diet is high in grains and legumes.
Plant foods contain phytates, which reduce zinc absorption.
Vegetarians and vegans can absolutely maintain good zinc status, but it requires a little more intention.
Helpful plant sources include:
pumpkin seeds
sesame seeds or tahini
cashews
chickpeas
lentils
hemp seeds
Traditional preparation methods such as soaking, sprouting and fermenting help improve mineral absorption from plant foods.
Does fish oil provide zinc?
No.
Omega-3 fish oils contain fatty acids such as EPA and DHA, but they do not provide meaningful amounts of zinc. Minerals remain in the tissue of the food, not in the extracted oil.
Whole foods provide minerals. Oils provide fats.
Both have their place, but they are not interchangeable.
Should zinc be taken with copper?
Zinc and copper work together in the body and need to remain balanced.
Taking higher doses of zinc for long periods can gradually reduce copper absorption. Copper is important for iron metabolism, connective tissue health and nervous system function.
For this reason, many practitioners recommend ensuring copper intake remains adequate when zinc is supplemented for several months.
Nature often balances these minerals together in foods such as shellfish, nuts and organ meats.
Choosing a zinc supplement
If supplementation is needed, some of the better absorbed forms include:
zinc picolinate
zinc bisglycinate
zinc citrate
These tend to be easier for the body to absorb than zinc oxide.
For many adults, 15–25 mg daily is a common supportive range, though individual needs can vary.
Higher doses are sometimes used short term but should be approached thoughtfully.
How long should zinc be taken?
For general support, zinc can often be taken daily for a few months, then reviewed.
A practical approach used by many people is:
2 to 3 months of supplementation
followed by a short break or reassessment
This is especially wise if symptoms improve, diet changes, or the person is also using a multi-mineral formula.
As always, the goal is not to live by the supplement drawer like it is a tiny pharmacy in the kitchen. The real aim is to restore balance and support the body well enough that it needs less propping up over time.
A final thought
Zinc may not be the most glamorous nutrient, but it is one of the most important.
It influences immunity, digestion, brain chemistry, sleep, stress resilience, hormone function and tissue repair. When it is low, the body often sends out early whispers long before it starts shouting.
For those who cannot eat shellfish, oysters or red meat, zinc is worth paying attention to. For those under chronic stress, struggling with poor sleep, frequent infections or slow recovery, it may be one of the missing pieces.
As with so much in health, the body works as an integrated system. Zinc does not act alone, but without it, many systems begin to falter.
Sometimes the smallest minerals carry the biggest workload.
Disclaimer: The information provided in this article is for educational and informational purposes only and is not intended as medical advice. It should not be used to diagnose, treat, cure, or prevent any medical condition. Always consult with a qualified healthcare professional before starting any new supplement, nutritional programme, or health intervention, particularly if you have an existing medical condition, are pregnant, breastfeeding, or taking prescription medications.
Individual nutritional needs can vary, and what is appropriate for one person may not be suitable for another.
This article is intended to support informed health awareness and should not replace personalised medical guidance.
I hope you feel inspired. Look after your body, and it will keep you healthy.
Catherine
CWD 16 March 2026/Ireland
About the Author
Dr. Catherine W. Dunne MSc.D., RGN is a nurse, holistic practitioner, and educator based in Wexford, Ireland. With over 30 years of experience in healthcare and energy-based healing modalities, she integrates conventional medical knowledge with holistic approaches to support whole-person well-being.
Catherine is the founder of Holistic HealthCare Wexford and co-founder of Aumvedas Academy, where she teaches courses in holistic health, energy medicine, and integrative healing practices.
Her work focuses on empowering people to understand the body as an intelligent system capable of healing when supported with the right knowledge, nutrition, and energetic balance.
For many years we were told something simple about bone health:
By Dr Catherine W. Dunne MSc.D., RGN Holistic HealthCare Wexford & Aumvedas Academy Nurse, Medical Intuitive and Holistic Practitioner
Take calcium and a little vitamin D.
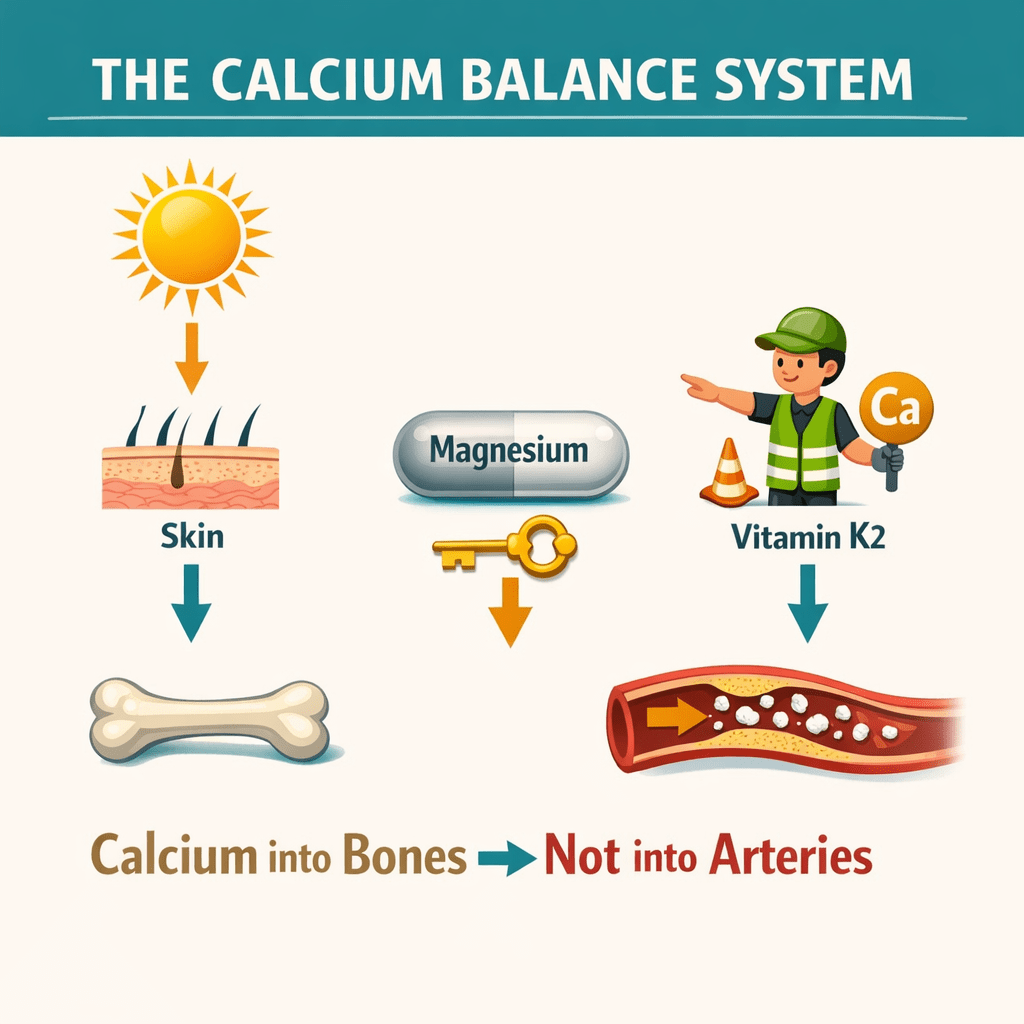
But modern research is showing that calcium metabolism is far more sophisticated than that. The body relies on a small team of nutrients working together — most importantly vitamin D3, magnesium and vitamin K2.
When these nutrients are balanced, calcium is more likely to support healthy bones rather than accumulating in places where it should not be.
Understanding how this system works can help us make better choices for long-term health.
What do vitamin D3, magnesium and vitamin K2 do together?
Vitamin D3 helps the body absorb calcium from food, magnesium activates vitamin D so it can function properly, and vitamin K2 directs calcium into bones while helping prevent deposits in arteries and soft tissues. Together, these nutrients support healthy calcium balance, bone strength and overall metabolic health.
Vitamin D3 – The Sunshine Signal
Vitamin D is often called a vitamin, but in reality it behaves more like a hormone.
Production begins in the skin when ultraviolet-B sunlight converts a cholesterol-related molecule called 7-dehydrocholesterol into vitamin D3.
Once activated by the liver and kidneys, vitamin D influences hundreds of genes involved in:
• calcium absorption • immune regulation • inflammation control • muscle strength • bone metabolism
One of its most important roles is helping the body absorb calcium from food.
Without sufficient vitamin D, the body may absorb only a small fraction of the calcium we eat.
Low vitamin D levels have also been associated in research studies with a range of conditions including:
• osteoporosis • autoimmune diseases such as multiple sclerosis • certain cancers including breast and bowel cancer.
This does not mean vitamin D alone prevents these diseases, but it highlights how important it is in maintaining normal physiological balance.
Magnesium – The Quiet Enabler
Here is a fact that many people do not realise.
Vitamin D cannot function properly without magnesium.
Magnesium is required for the enzymes that activate vitamin D in the body. Without adequate magnesium, vitamin D may remain largely inactive.
Magnesium also plays important roles in:
• parathyroid hormone regulation • nerve and muscle function • heart rhythm stability • bone mineralisation.
Unfortunately magnesium deficiency has become common in modern diets due to soil depletion, processed foods and certain medications.
When magnesium levels are low, increasing calcium intake alone often fails to correct imbalances.
Vitamin K2 – The Calcium Guide
If vitamin D increases calcium absorption, another important question arises:
Where does that calcium go?
Vitamin K2 helps answer that question.
This nutrient activates specialised proteins that guide calcium into the bones while helping prevent calcium deposits in arteries and soft tissues.
Two important vitamin K2-dependent proteins include:
• Osteocalcin, which binds calcium into the bone matrix • Matrix GLA protein, which helps prevent vascular calcification.
In simple terms, vitamin K2 acts like a traffic controller for calcium, helping ensure it strengthens bones rather than accumulating where it does not belong.
Why Calcium From Food Is Often Preferable
Calcium is clearly important for bone health, but more is not always better.
Many people can obtain adequate calcium through foods such as:
• dairy products • leafy green vegetables • almonds and sesame seeds • small fish eaten with bones.
Supplements may be appropriate in certain situations, but high calcium intake without sufficient vitamin D, magnesium and K2 may not support healthy calcium balance.
For this reason, many clinicians now emphasise dietary calcium alongside nutrient balance rather than relying solely on supplements.
Vitamin D and the Immune System
Beyond bone health, vitamin D plays an important role in immune regulation.
Immune cells contain vitamin D receptors, and adequate levels appear to help maintain balanced immune responses.
Researchers have explored links between vitamin D status and conditions such as:
• multiple sclerosis • autoimmune diseases • breast cancer • colorectal (bowel) cancer.
While vitamin D is not a treatment for these conditions, maintaining healthy levels may support the body’s natural defence systems.
Interestingly, the prevalence of multiple sclerosis increases in populations living further from the equator, where sunlight exposure — and therefore vitamin D production — is lower.
A Simple Way to Think About the System
Instead of focusing on a single nutrient, it helps to think of calcium regulation as a partnership.
Vitamin D3 helps the body absorb calcium.
Magnesium activates vitamin D and supports metabolic processes.
Vitamin K2 directs calcium into bones and away from soft tissues.
Calcium provides the structural building blocks for bones and teeth.
When these nutrients work together, the body is better able to maintain balance.
Diagram showing how Vitamin D3, magnesium and vitamin K2 work together to regulate calcium and support bone health.
Supporting Healthy Nutrient Levels
Some practical ways to support this system include:
• sensible sunlight exposure where possible • eating a varied diet rich in vegetables, nuts and seeds • including fermented foods or high-quality dairy where tolerated • discussing testing or supplementation with a healthcare professional when appropriate.
Every individual is different, and personalised guidance is always best.
Health rarely depends on one nutrient or one supplement.
The body works through networks of nutrients and signals, each supporting the other.
Understanding how vitamin D3, magnesium and vitamin K2 interact gives us a clearer picture of how the body manages calcium, supports bone health and maintains overall wellbeing.
Sometimes the most effective approach is simply helping the body restore its natural balance.
I hope you feel inspired. Look after your body, and it will keep you healthy.
Catherine
CWD 14 March 2026/Ireland
Dr Catherine W. Dunne MSc.D., RGN, M.H.I.T. is a nurse, holistic practitioner, and educator based in Wexford, Ireland. With over 35 years of experience in healthcare and energy-based healing modalities, she integrates conventional medical knowledge with holistic approaches to support whole-person well-being.
Catherine is the founder of Holistic HealthCare Wexford and co-founder of Aumvedas Academy, where she teaches courses in holistic health, energy medicine, and integrative healing practices.
Her work focuses on empowering people to understand the body as an intelligent system capable of healing when supported with the right knowledge, nutrition, and energetic balance.
Learn more: Holistic HealthCare Wexford Aumvedas Academy
Disclaimer
The information provided in this article is for educational purposes only and is not intended as medical advice. Always consult a qualified healthcare professional before starting any new supplement or health intervention.
By Dr. Catherine W. Dunne | Holistic HealthCare Wexford & Aumvedas Academy Dr Catherine W Dunne MSc. D., RGN, Reiki Master (RGMT), M.H.I.T: Master Acupressure. Practitioner of Reflexology. Expert in Aromatherapy. Specialized in Deep Tissue/Myo-fascia Massages. Proficient in Infrared Treatments. Vibrational Sound and Colour Therapist. Tissue Salt Advisor. Pendulum Healing Dowser. Chakra Practitioner. Tao Cosmic Healing Practitioner. Practitioner of Plant and Herb Medicine and licensed Nurse.
Fanta Zero, Coca-Cola Zero, 7-Up Free, Sprite Zero, Lucozade Zero, Pepsi Max and their likes. Here is a little research I have done for you.
I am looking at the health impact of Zero Diet Sodas and what damage they cause to our body.
“Zero” sodas are marketed as the healthier option because they contain no sugar, no calories, no guilt. But does zero sugar really mean zero impact on health?
The short answer is no.
Let’s look at what’s actually inside these drinks and how they affect the body — particularly the kidneys, bones, metabolism, and gut.
What Are “Zero” Sodas? “Zero” or diet sodas remove sugar and calories, replacing them with artificial sweeteners and acids to preserve sweetness and flavour. They typically contain:
Carbonated water
Artificial sweeteners (most commonly aspartame, often combined with acesulfame-K)
Acids (citric acid or phosphoric acid)
Flavourings
They are called “Zero” because they contain no calories, not because they are biologically neutral.
Aspartame: The Ingredient Most People Don’t Question Most Zero sodas contain aspartame. Aspartame breaks down in the body into:
Phenylalanine
Aspartic acid
Small amounts of methanol
In occasional use, aspartame is generally tolerated by healthy adults. Concerns arise with regular, long-term daily consumption.
Effects on the Kidneys Large population studies consistently show that frequent diet soda consumption is associated with:
Faster decline in kidney function (eGFR)
Increased risk of chronic kidney disease
Higher rates of hypertension and metabolic stress
These effects are not caused by carbonation, but are likely related to:
Changes in gut microbiota
Increased oxidative stress
Insulin and blood-pressure dysregulation
Chronic low-grade inflammation
Plain sparkling water does not show these associations.
Effects on Bone Health Many Zero sodas — particularly colas — still contain phosphoric acid. High phosphorus intake without adequate calcium can:
Disrupt calcium balance
Increase calcium loss through urine
Reduce bone mineral density over time
Long-term diet soda consumption has been linked to lower bone density, especially in post-menopausal women.
Again, these effects are not seen with plain fizzy water.
Effects on Metabolism and Appetite Despite being calorie-free, artificial sweeteners can:
Trigger insulin release in some individuals
Disrupt hunger and satiety signalling
Increase cravings for sweet foods later
Alter dopamine reward pathways
In practice, many people who consume diet sodas regularly do not lose weight, and some gain weight over time.
The body does not like being tricked.
Effects on Gut Health Artificial sweeteners can alter gut bacteria, leading to:
Reduced glucose tolerance
Increased inflammatory signalling
Impaired mineral absorption
Gut health plays a direct role in kidney health, bone health, and metabolic balance.
What “Zero” Sodas Are — and Are Not
✔ Better than sugar-sweetened sodas ✖ Not kidney-protective ✖ Not bone-supportive ✖ Not metabolically neutral
They remove sugar, not physiological consequences.
Who Should Be Especially Careful? This is something no General Practitioner (GP)/Family Doctor or Hospital Consultant tells you. Regular consumption of Zero sodas is best avoided in people with:
Kidney disease or reduced kidney function
Hypertension
Osteopenia or osteoporosis
Diabetes or insulin resistance
Migraine disorders
Gut sensitivity or IBS
Healthier Alternatives If you enjoy fizz:
Sparkling mineral water
Sparkling water with lemon or lime
Herbal iced teas
Kombucha (in moderation)
If you want sweetness:
Small amounts of real juice diluted with sparkling water – this is what I like doing.
The Bottom Line Zero sodas are not toxic, but they are not health drinks.
An occasional one is unlikely to cause harm. A daily habit over years is where issues quietly accumulate.
Zero calories does not mean zero impact.
I hope you feel inspired. Look after your body, and it will keep you healthy.
By Dr Catherine W Dunne MSc. D., RGN, Reiki Master (RGMT), M.H.I.T: Master Acupressure, Practitioner of Reflexology, Aromatherapy, Deep Tissue/Myo-fascia Massages, Infrared Treatments, Vibrational Sound and Colour Therapist, Tissue Salt Advisor, Pendulum Healing Dowser, Chakra Practitioner , Tao Cosmic Healing Practitioner, Practitioner of Plant and Herb Medicine and Nurse.
Vitamin D – the right intake
Taking vitamin D is an excellent preventive but also therapeutic measure. Regardless of whether it is an increased susceptibility to infections, autoimmune diseases, degenerative complaints or problems such as diabetes, high blood pressure, depression and dementia, a vitamin D deficiency is usually the cause of the action. We explain how you can determine a vitamin D deficiency in the home test, how much vitamin D you need and how you can properly combine vitamin D with calcium, magnesium and vitamin K.
Vitamin D – How to take it correctly?
Vitamin D is particularly known for its bone-strengthening effect. It promotes calcium absorption from the intestine, is involved in calcium incorporation into the bones, inhibits bone loss and also strengthens the immune system.
At the same time, there is hardly a disease that does not develop Vitamin D deficiency would be involved. For example, the vitamin is considered a substance with an anti-inflammatory effect, which alone is reason enough for its positive influence in most chronic complaints – because they all go hand in hand with chronically inflammatory processes.
It is therefore important to pay attention to a healthy vitamin D level. How do you do that? Does the vitamin have to be taken as a dietary supplement? And if so, what is the right income? How to calculate the personally required dose and how to combine the vitamin with calcium, magnesium and Vitamin K?
A deficiency is common
Vitamin D is not a real vitamin. Because real vitamins must be ingested with food. With vitamin D, on the other hand, the body can also supply itself solely through the sun’s rays, since the vitamin is formed in the skin under the influence of UVB radiation.
However, in Central Europe this only works in summer (from around April to September) – and only if you are lightly dressed and do not constantly apply sunscreens with a high sun protection factor. The latter can reduce vitamin D formation in the skin. In Northern Europe you will need to supplement all year round,
The rest of the year, the sun is too low to send enough UVB radiation to Earth. In Central Europe you can only get along well with the help of the sun Vitamin D if you are really in the open air in the warm season to fill up your memories so comprehensively that you can get over the winter well.
However, many people do not succeed in what the modern lifestyle with an hourly stay in closed rooms is not entirely innocent. Therefore, large sections of the population suffer from vitamin D deficiency and should take the vitamin especially in winter.
Vitamin D is a fat-soluble vitamin
The bone vitamin belongs together with vitamin A, Vitamin E. and Vitamin K to the fat-soluble vitamins. That means two things:
There is always something for the absorption of vitamin D from the intestine fat required (see below under “Correct intake: Always with a little fat”).
The vitamin can be stored in the body (in adipose tissue and in the liver), which is almost never the case with water-soluble vitamins (B, C).
The advantage is that you don’t have to take vitamin D – once the stores are filled – every day. The organism can draw from a filled store for weeks or even months.
The disadvantage is that fat-soluble vitamins can also be overdosed, which you have to pay attention to when taking them. Because while excess water-soluble vitamins are usually simply discharged through the urine, this is not the case with fat-soluble vitamins. Cases of vitamin A overdoses are therefore known from time to time, for example from regions where fish liver is often eaten. This contains a lot of Vitamin A.
What dose leads to overdose?
As far as vitamin D is concerned, there is usually only the risk of an overdose if very high doses in the form of nutritional supplements are taken over a longer period of time.
50 µg or 2,000 IU per day are the recommended maximum dose in Europe and North America. However, clinical studies show that long-term intake of 10,000 IU daily does not pose any risks. An overdose could occur at 50,000 IU per day and at serum values of more than 150 ng / ml. Wa can then form hypercalcemia (too much calcium in the blood) – such an evaluation by Indian researchers from May 2011 in Oman Medical Journal.
Ideally, the blood values of vitamin D should be below 100 ng / ml, since primitive people rarely reach higher values, even though they are not dressed in the sun every day. The toxic range clearly begins at 300 ng / ml.
Overdose: from 50,000 IU per day for several months
Various case reports have also become known from 2011, in which an overdose of vitamin D led to complaints.
In a 70-year-old woman who took 50,000 IU daily, the typical symptoms of hypercalcemia occurred after 3 months of taking it: tiredness, walking difficulties and confusion. After stopping vitamin D, however, it recovered completely over the course of five months. It should be noted here that she also consumed over 3 g of calcium daily.
Another case describes a man in whom accidentally taking 2,000,000 IU of vitamin D a day after 2 months led to confusion, exhaustion, excessive thirst and frequent urination.
And in a third case, after taking 50,000 IU of vitamin D daily for six months, a man also observed the typical symptoms of hypercalcemia:
Excessive thirst and frequent urination
Stomach discomfort, Nausea, vomiting and constipation
Bone pain, muscle weakness
Confusion, lethargy and exhaustion
Overdose from food or sun?
Since vitamin D hardly occurs in food, you can hardly eat an overdose (unless you eat a lot of fish liver).
It is also hardly possible to get an overdose from the sun’s rays. Apparently, the body has protective measures that stop vitamin D formation via the skin as soon as a sufficiently high serum value is reached.
On a sunny summer day, the body rarely absorbs more than 10,000 IU of vitamin D in –, and only if you spent the whole day almost undressed (bath pants / bikini) in the sun.
Only in extreme sunlight (for years in hot regions all day on the beach) could there be unfavorable consequences of an overdose of vitamin D, but only here if there is a vitamin K2 deficiency and possibly too well-intentioned calcium supply at the same time.
So it is rather the over-dosed intake of the vitamin in the form of a dietary supplement that could lead to problems.
Make vitamin D preparation from mushrooms and sun yourself
We have described here how you can produce a natural source of vitamins from mushrooms: Pure vegetable vitamin source: mushrooms
Of course, this method cannot be used specifically to achieve a certain value in the blood or to remedy a deficiency, since one does not know the actual vitamin D content of the fungi, but one can prepare them accordingly Edible mushrooms Install regularly in the diet, so that in the long term you only have to take low-dose supplements or at some point no more.
The right intake
Below we describe all the factors you need to know for a correct intake of vitamin D. First, it is about which four vital substances the vitamin needs to work properly, then how you measure your vitamin D level and finally we present two methods with which you can find out or calculate the dose that suits you can.
1. Take vitamin K2
When taking vitamin D, it is always recommended to pay attention to a healthy vitamin K2 supply at the same time. Vitamin K2 is the vitamin that fulfills two major tasks in the body:
Vitamin K is involved in regulating blood clotting so that no one has to bleed to the smallest wound.
Vitamin K conducts excess calcium in the blood into the bones, thus ensuring that the calcium is not deposited on the blood vessel walls or in the form of kidney stones.
Since vitamin D promotes the absorption of calcium, the amount of calcium absorbed also increases when the vitamin is taken. If vitamin K2 is now missing, the problems mentioned above can arise, i.e. a misdistribution of calcium in the body.
A 2015 study showed in kidney patients that the combined administration of vitamin D and vitamin K reduced the progression of arteriosclerosis (compared to the group that only received sun vitamin).
It is not entirely clear how much vitamin K2 you should take. The recommended doses for vitamin D supplementation vary considerably among experts. Information can be found there, such as B.
Taking 100 µg vitamin K2 per 5,000 IU vitamin D
Ingestion of 100 µg vitamin K2 per 10,000 IU
Ingestion of 100 µg vitamin K2 per 1,000 IU
There is also a recommendation depending on body weight: 2 – 3 µg vitamin K2 per kilogram of body weight.
We recommend taking vitamin K2 the following
Ingestion of 100 µg vitamin K2 at up to 2,500 IU vitamin D per day
Ingestion of 200 µg vitamin K2 in vitamin D doses above 2,500 IU per day
However, also note the vitamin K2 content of your food. If you adapt your diet accordingly and now take in enough vitamin K2 from your diet, you may only have to take vitamin K2 in the first weeks of your vitamin D intake until the stores are replenished and your diet then provides the required vitamin.
Vitamin K2 is available in various forms, we recommend taking Menachinon-7, which is also abbreviated as MK-7. It is vegan and is considered the best resorbable and usable vitamin K2 form.
If you are on a blood thinner or taking other medications that are not so well compatible with vitamin K, the correct intake of vitamin K must be discussed with the doctor as a precaution.
2nd Vitamin A increases the effect
In the presence of vitamin A, vitamin D works better, and the vitamin D level rises higher if vitamin A is taken at the same time – at least one study from August 2020. Read information about this in our article Vitamin D needs vitamin A.. The correct intake of vitamin D therefore also includes vitamin A (about 1 mg per day).
Vitamin A can be ingested via beta-carotene, which is contained in many types of vegetables, because the organism can produce vitamin A from beta-carotene. To do this, however, you should eat vegetables rich in beta-carotene every day, because to produce 1 mg of vitamin A, the organism needs at least 6 times the amount of beta-carotene, i.e. 6 mg. The following vegetables are among the best sources of beta carotene (quantities always per 100 g):
Carrots raw 9.8 mg beta-carotene (1.6 mg vitamin A)
Spinach raw 4.7 mg beta-carotene (0.8 mg vitamin A)
Kale raw 5.1 mg beta-carotene (0.8 mg vitamin A)
Corn salad raw 3.9 mg beta-carotene (0.65 mg vitamin A)
red peppers raw 2.1 mg beta-carotene (0.35 mg vitamin A)
When cooking, the content does not change noticeably because beta-carotene is not sensitive to heat; bioavailability could even increase due to cooking – see details here: Loss of nutrients when cooking where we explain what you need to look out for when preparing in order to benefit as much as possible from the beta-carotene it contains.
In the study mentioned, the vitamin A level of the participants was originally even normal. Nevertheless, taking vitamin A (together with taking vitamin D) resulted in a higher vitamin D level and also an improved effect of the vitamin.
In particular in the case of acute diseases and at the same time there is a D deficiency or even if the value should not increase satisfactorily despite all efforts, the additional intake of vitamin A or Beta Carotin can be a good help.
3rd Magnesium activates vitamin D.
Since magnesium is required in the body to activate vitamin D and is also consumed in this process, the correct intake of vitamin D also requires an optimized magnesium supply.
The daily requirement for magnesium is about 400 mg for an adult. If you take up this amount of magnesium daily through your diet, you should be well looked after with a vitamin D supplementation of up to 5,000 IU.
However, if you take more vitamin D, you should also take magnesium with this higher dose, between 200 – 300 mg – depending on the magnesium content of the diet. Read details here: Low magnesium levels make Vitamin D ineffective.
Magnesium is the fourth most abundant mineral in the human body after calcium, potassium, and sodium. Foods high in magnesium include almonds, bananas, beans, broccoli, brown rice, cashews, egg yolk, fish oil, flaxseed, green vegetables, milk, mushrooms, other nuts, oatmeal, pumpkin seeds, sesame seeds, soybeans, sunflower seeds, sweet corn, tofu, and whole grains.
4th Vitamin D and calcium are only advisable in certain situations
Vitamin D is considered to be THE bone vitamin par excellence, and it is often believed that the correct intake includes calcium in any case. But this only seems to make sense in certain cases:
if e.g. B. the risk of osteoporosis should be reduced in the menopause
if osteoporosis is already present and the risk of bone fracture is to be reduced
when a low-calcium diet is practiced that delivers significantly less than the 1,000 mg calcium recommended daily
However, if you consume sufficient calcium, you should not take any additional calcium when taking vitamin D (especially at very high doses). This could increase the risk of hypercalcemia.
Correct intake: Measure vitamin D levels in advance!
Proper intake of vitamin D can only take place if you know your actual value and can then calculate the dose that suits you individually or get it said by your doctor.
So get your vitamin D level established first. Otherwise, you may take too little and therefore have no effect. Or you take much more than necessary, which in turn would put unnecessary strain on your body.
Your family doctor (GP), or alternative practitioner can take care of the measurement. You can also do a vitamin D home test yourself at home. For safety’s sake, you should also discuss the result with a doctor or Integrated Medical Practitioner/CAM Practitioner.
Your qualified Integrated Medical Practitioner/CAM Practitioner can also perform a simple test. But do ask your GP/Family Doctor if he/she can request the laboratory test.
However, the blood drawn itself can have influences on the blood that falsify the result. It is therefore safer to have the test done by the doctor or alternative practitioner.
Correct intake: what dose?
The goal should be a blood value of at least 30 ng / ml, better about 40 to 50 ng / ml vitamin D3 (25 (OH) vitamin D3). The dose that suits you is now calculated from your current value and your desired value –, taking into account the body weight.
In the event of a massive deficiency, the procedure described in the article linked above could not lead to a healthy vitamin D level quickly enough. Therefore we provide you with the method according to Dr. med. Raimund von Helden, author of the recommended booklet Healthy in seven days – Success with vitamin D therapy.
Dr. von Helden divides the intake of vitamin D into two therapeutic parts: into the initial therapy and the permanent or Maintenance therapy.
After a deficiency, the initial therapy serves to fill up the vitamin D stores, which should happen as quickly as possible so that the mostly existing deficiency symptoms can be remedied as quickly as possible. It is a single dose. The dose of continuous therapy is then switched over.
The continuous therapy provides the amount of vitamin D that is required to compensate for the daily losses and to maintain a healthy vitamin D level in the long term.
Calculation of the dose for the initial therapy
In order to raise the vitamin D level by 1 ng / ml, 10,000 IU are required with a body weight of 70 kilograms. If the body weight is different, recalculate the value proportionally. 7,000 IU per kilogram of body weight should not be exceeded.
For example, if you weigh 70 kg, have an instantaneous value of 15 ng / ml and want to reach a value of 35 ng / ml, then choose a single dose of 200,000 IU as the initial therapy. Weigh only 60 kg, then take about 170,000 IU.
The starting dose is very high. We recommend that you discuss this type of intake with the doctor or alternative practitioner in advance.
Calculation of the dose for continuous therapy
With an assumed body weight of 70 kilograms in turn, 3,333 IU of vitamin D per day or 23,000 IU required per week. Here, too, the dose is calculated proportionally with a different body weight. For the average person in Ireland we can say 5000IU vitamin D per day
If you are in the sun a lot in summer, you can pause with vitamin D during this time. But probably no alarmingly high value would develop if you continued to take it despite sunbathing.
Correct intake: Always with a little fat
If you have vitamin D preparations that are available as powder in capsules if taken with black coffee, water or juice, this leads to absorption of the vitamin, but to a rather low absorption. As a fat-soluble vitamin, vitamin D should always be taken with a little fat. Like a glass of milk or Cholesterol lowering milk drinks or joghurt.
Too much fat is not a good idea either. So if you take the vitamin preparation with a thick lard bread or fatty cheese, you cannot take the ideal dose of it either. Because excessive amounts of fat seem to inhibit absorption.
A 2013 study found that taking vitamin D with 11 grams of fat resulted in absorption 16 percent higher than taking with 35 grams of fat and 20 percent higher absorption than taking with 0 grams of fat.
It doesn’t matter whether you get fat out polyunsaturated fatty acids (Hemp oil, Linseed oil, Sunflower oil), one made from monounsaturated fatty acids (olive oil, Avocados, Almonds) or one made of saturated (coconut oil).
Correct intake: Topical via the skin
If you cannot tolerate vitamin D preparations or whose vitamin D level simply does not want to rise despite the correct intake of vitamin D preparations, the vitamin can also be applied to the skin, since it can also be absorbed through the skin.
To do this, choose a liquid preparation without unfavourable additives, e.g. Vitamin D3 drops, which only come from vitamin D3 and MCT fats (medium-chain fats from e.g. Coconut oil) exist. Apply to the forearm, where the skin is particularly receptive
Important note
Disclaimer: This article was based on (at the time of publication) current studies written and checked by doctors, but may not be used for self-diagnosis or self-treatment, replaced so not to visit your doctor. So, discuss each one Measure (whether from this or another of our articles) always first with your doctor.
Vitamin D – the right intake
Taking vitamin D is an excellent preventive but also therapeutic measure. Regardless of whether it is an increased susceptibility to infections, autoimmune diseases, degenerative complaints or problems such as diabetes, high blood pressure, depression and dementia, a vitamin D deficiency is usually the cause of the action. We explain how you can determine a vitamin D deficiency in the home test, how much vitamin D you need and how you can properly combine vitamin D with calcium, magnesium and vitamin K.
Vitamin D – How to take it correctly?
Vitamin D is particularly known for its bone-strengthening effect. It promotes calcium absorption from the intestine, is involved in calcium incorporation into the bones, inhibits bone loss and also strengthens the immune system.
At the same time, there is hardly a disease that does not develop Vitamin D deficiency would be involved. For example, the vitamin is considered a substance with an anti-inflammatory effect, which alone is reason enough for its positive influence in most chronic complaints – because they all go hand in hand with chronically inflammatory processes.
It is therefore important to pay attention to a healthy vitamin D level. How do you do that? Does the vitamin have to be taken as a dietary supplement? And if so, what is the right income? How to calculate the personally required dose and how to combine the vitamin with calcium, magnesium and Vitamin K?
(If you are for the Vitamin D blood values If you are interested in what value indicates a deficiency and which is just correct, read the link above (under Vitamin D).)
A deficiency is common
Vitamin D is not a real vitamin. Because real vitamins must be ingested with food. With vitamin D, on the other hand, the body can also supply itself solely through the sun’s rays, since the vitamin is formed in the skin under the influence of UVB radiation.
However, in Central Europe this only works in summer (from around April to September) – and only if you are lightly dressed and do not constantly apply sunscreens with a high sun protection factor. The latter can reduce vitamin D formation in the skin.
The rest of the year, the sun is too low to send enough UVB radiation to Earth. In Central Europe you can only get along well with the help of the sun Vitamin D if you are really in the open air in the warm season to fill up your memories so comprehensively that you can get over the winter well.
However, many people do not succeed in what the modern lifestyle with an hourly stay in closed rooms is not entirely innocent. Therefore, large sections of the population suffer from vitamin D deficiency and should take the vitamin especially in winter.
Vitamin D is a fat-soluble vitamin
The bone vitamin belongs together with vitamin A, Vitamin E. and Vitamin K to the fat-soluble vitamins. That means two things:
There is always something for the absorption of vitamin D from the intestine fat required (see below under “Correct intake: Always with a little fat”).
The vitamin can be stored in the body (in adipose tissue and in the liver), which is almost never the case with water-soluble vitamins (B, C).
The advantage is that you don’t have to take vitamin D – once the stores are filled – every day. The organism can draw from a filled store for weeks or even months.
The disadvantage is that fat-soluble vitamins can also be overdosed, which you have to pay attention to when taking them. Because while excess water-soluble vitamins are usually simply discharged through the urine, this is not the case with fat-soluble vitamins. Cases of vitamin A overdoses are therefore known from time to time, for example from regions where fish liver is often eaten. This contains a lot Vitamin A.
What dose leads to overdose?
As far as vitamin D is concerned, there is usually only the risk of an overdose if very high doses in the form of nutritional supplements are taken over a longer period of time.
50 µg or 2,000 IU per day are the recommended maximum dose in Europe and North America. However, clinical studies show that long-term intake of 10,000 IU daily does not pose any risks. An overdose could occur at 50,000 IU per day and at serum values of more than 150 ng / ml. Wa can then form hypercalcemia (too much calcium in the blood) – such an evaluation by Indian researchers from May 2011 in Oman Medical Journal.
Ideally, the blood values of vitamin D should be below 100 ng / ml, since primitive people rarely reach higher values, even though they are not dressed in the sun every day. The toxic range clearly begins at 300 ng / ml.
Overdose: from 50,000 IU per day for several months
Various case reports have also become known from 2011, in which an overdose of vitamin D led to complaints.
In a 70-year-old woman who took 50,000 IU daily, the typical symptoms of hypercalcemia occurred after 3 months of taking it: tiredness, walking difficulties and confusion. After stopping vitamin D, however, it recovered completely over the course of five months. It should be noted here that she also consumed over 3 g of calcium daily.
Another case describes a man in whom accidentally taking 2,000,000 IU of vitamin D a day after 2 months led to confusion, exhaustion, excessive thirst and frequent urination.
And in a third case, after taking 50,000 IU of vitamin D daily for six months, a man also observed the typical symptoms of hypercalcemia:
Excessive thirst and frequent urination
Stomach discomfort, Nausea, vomiting and constipation
Bone pain, muscle weakness
Confusion, lethargy and exhaustion
Overdose from food or sun?
Since vitamin D hardly occurs in food, you can hardly eat an overdose (unless you eat a lot of fish liver).
It is also hardly possible to get an overdose from the sun’s rays. Apparently, the body has protective measures that stop vitamin D formation via the skin as soon as a sufficiently high serum value is reached.
On a sunny summer day, the body rarely absorbs more than 10,000 IU of vitamin D in –, and only if you spent the whole day almost undressed (bath pants / bikini) in the sun.
Only in extreme sunlight (for years in hot regions all day on the beach) could there be unfavorable consequences of an overdose of vitamin D, but only here if there is a vitamin K2 deficiency and possibly too well-intentioned calcium supply at the same time.
So it is rather the over-dosed intake of the vitamin in the form of a dietary supplement that could lead to problems.
Make vitamin D preparation from mushrooms and sun yourself
We have described here how you can produce a natural source of vitamins from mushrooms: Pure vegetable vitamin source: mushrooms
Of course, this method cannot be used specifically to achieve a certain value in the blood or to remedy a deficiency, since one does not know the actual vitamin D content of the fungi, but one can prepare them accordingly Edible mushrooms Install regularly in the diet, so that in the long term you only have to take low-dose supplements or at some point no more.
The right intake
Below we describe all the factors you need to know for a correct intake of vitamin D. First, it is about which four vital substances the vitamin needs to work properly, then how you measure your vitamin D level and finally we present two methods with which you can find out or calculate the dose that suits you can.
1. Take vitamin K2
When taking vitamin D, it is always recommended to pay attention to a healthy vitamin K2 supply at the same time. Vitamin K2 is the vitamin that fulfills two major tasks in the body:
Vitamin K is involved in regulating blood clotting so that no one has to bleed to the smallest wound.
Vitamin K conducts excess calcium in the blood into the bones, thus ensuring that the calcium is not deposited on the blood vessel walls or in the form of kidney stones.
Since vitamin D promotes the absorption of calcium, the amount of calcium absorbed also increases when the vitamin is taken. If vitamin K2 is now missing, the problems mentioned above can arise, i.e. a misdistribution of calcium in the body.
A 2015 study showed in kidney patients that the combined administration of vitamin D and vitamin K reduced the progression of arteriosclerosis (compared to the group that only received sun vitamin).
It is not entirely clear how much vitamin K2 you should take. The recommended doses for vitamin D supplementation vary considerably among experts. Information can be found there, such as B.
Taking 100 µg vitamin K2 per 5,000 IU vitamin D
Ingestion of 100 µg vitamin K2 per 10,000 IU
Ingestion of 100 µg vitamin K2 per 1,000 IU
There is also a recommendation depending on body weight: 2 – 3 µg vitamin K2 per kilogram of body weight.
We recommend taking vitamin K2 the following
Ingestion of 100 µg vitamin K2 at up to 2,500 IU vitamin D per day
Ingestion of 200 µg vitamin K2 in vitamin D doses above 2,500 IU per day
However, also note the vitamin K2 content of your food. If you adapt your diet accordingly and now take in enough vitamin K2 from your diet, you may only have to take vitamin K2 in the first weeks of your vitamin D intake until the stores are replenished and your diet then provides the required vitamin.
Vitamin K2 is available in various forms, we recommend taking Menachinon-7, which is also abbreviated as MK-7. It is vegan and is considered the best resorbable and usable vitamin K2 form.
If you are on a blood thinner or taking other medications that are not so well compatible with vitamin K, the correct intake of vitamin K must be discussed with the doctor as a precaution.
2nd Vitamin A increases the effect
In the presence of vitamin A, vitamin D works better, and the vitamin D level rises higher if vitamin A is taken at the same time – at least one study from August 2020. Read information about this in our article Vitamin D needs vitamin A.. The correct intake of vitamin D therefore also includes vitamin A (about 1 mg per day).
Vitamin A can be ingested via beta-carotene, which is contained in many types of vegetables, because the organism can produce vitamin A from beta-carotene. To do this, however, you should eat vegetables rich in beta-carotene every day, because to produce 1 mg of vitamin A, the organism needs at least 6 times the amount of beta-carotene, i.e. 6 mg. The following vegetables are among the best sources of beta carotene (quantities always per 100 g):
Carrots raw 9.8 mg beta-carotene (1.6 mg vitamin A)
Spinach raw 4.7 mg beta-carotene (0.8 mg vitamin A)
Kale raw 5.1 mg beta-carotene (0.8 mg vitamin A)
Corn salad raw 3.9 mg beta-carotene (0.65 mg vitamin A)
red peppers raw 2.1 mg beta-carotene (0.35 mg vitamin A)
When cooking, the content does not change noticeably because beta-carotene is not sensitive to heat; bioavailability could even increase due to cooking – see details here: Loss of nutrients when cooking where we explain what you need to look out for when preparing in order to benefit as much as possible from the beta-carotene it contains.
In the study mentioned, the vitamin A level of the participants was originally even normal. Nevertheless, taking vitamin A (together with taking vitamin D) resulted in a higher vitamin D level and also an improved effect of the vitamin.
In particular in the case of acute diseases and at the same time there is a D deficiency or even if the value should not increase satisfactorily despite all efforts, the additional intake of vitamin A or Beta Carotin can be a good help.
3rd Magnesium activates vitamin D.
Since magnesium is required in the body to activate vitamin D and is also consumed in this process, the correct intake of vitamin D also requires an optimized magnesium supply.
The daily requirement for magnesium is about 400 mg for an adult. If you take up this amount of magnesium daily through your diet, you should be well looked after with a vitamin D supplementation of up to 5,000 IU.
However, if you take more vitamin D, you should also take magnesium with this higher dose, between 200 – 300 mg – depending on the magnesium content of the diet. Read details here: Low magnesium levels make Vitamin D ineffective.
Magnesium is the fourth most abundant mineral in the human body after calcium, potassium, and sodium. Foods high in magnesium include almonds, bananas, beans, broccoli, brown rice, cashews, egg yolk, fish oil, flaxseed, green vegetables, milk, mushrooms, other nuts, oatmeal, pumpkin seeds, sesame seeds, soybeans, sunflower seeds, sweet corn, tofu, and whole grains.
4th Vitamin D and calcium are only advisable in certain situations
Vitamin D is considered to be THE bone vitamin par excellence, and it is often believed that the correct intake includes calcium in any case. But this only seems to make sense in certain cases:
if e.g. B. the risk of osteoporosis should be reduced in the menopause
if osteoporosis is already present and the risk of bone fracture is to be reduced
when a low-calcium diet is practiced that delivers significantly less than the 1,000 mg calcium recommended daily
However, if you consume sufficient calcium, you should not take any additional calcium when taking vitamin D (especially at very high doses). This could increase the risk of hypercalcemia.
Correct intake: Measure vitamin D levels in advance!
Proper intake of vitamin D can only take place if you know your actual value and can then calculate the dose that suits you individually or get it said by your doctor.
So get your vitamin D level established first. Otherwise, you may take too little and therefore have no effect. Or you take much more than necessary, which in turn would put unnecessary strain on your body.
Your family doctor (GP), or alternative practitioner can take care of the measurement. You can also do a vitamin D home test yourself at home. For safety’s sake, you should also discuss the result with a doctor or Integrated Medical Practitioner/CAM Practitioner.
Your qualified Integrated Medical Practitioner/CAM Practitioner can also perform a simple test. But do ask your GP/Family Doctor if he/she can request the laboratory test.
However, the blood drawn itself can have influences on the blood that falsify the result. It is therefore safer to have the test done by the doctor or alternative practitioner.
Correct intake: what dose?
The goal should be a blood value of at least 30 ng / ml, better about 40 to 50 ng / ml vitamin D3 (25 (OH) vitamin D3). The dose that suits you is now calculated from your current value and your desired value –, taking into account the body weight.
In the event of a massive deficiency, the procedure described in the article linked above could not lead to a healthy vitamin D level quickly enough. Therefore we provide you with the method according to Dr. med. Raimund von Helden, author of the recommended booklet Healthy in seven days – Success with vitamin D therapy.
Dr. von Helden divides the intake of vitamin D into two therapeutic parts: into the initial therapy and the permanent or Maintenance therapy.
After a deficiency, the initial therapy serves to fill up the vitamin D stores, which should happen as quickly as possible so that the mostly existing deficiency symptoms can be remedied as quickly as possible. It is a single dose. The dose of continuous therapy is then switched over.
The continuous therapy provides the amount of vitamin D that is required to compensate for the daily losses and to maintain a healthy vitamin D level in the long term.
Calculation of the dose for the initial therapy
In order to raise the vitamin D level by 1 ng / ml, 10,000 IU are required with a body weight of 70 kilograms. If the body weight is different, recalculate the value proportionally. 7,000 IU per kilogram of body weight should not be exceeded.
For example, if you weigh 70 kg, have an instantaneous value of 15 ng / ml and want to reach a value of 35 ng / ml, then choose a single dose of 200,000 IU as the initial therapy. Weigh only 60 kg, then take about 170,000 IU.
The starting dose is very high. We recommend that you discuss this type of intake with the doctor or alternative practitioner in advance.
Calculation of the dose for continuous therapy
With an assumed body weight of 70 kilograms in turn, 3,333 IU of vitamin D per day or 23,000 IU required per week. Here, too, the dose is calculated proportionally with a different body weight. For the average person in Ireland we can say 5000IU vitamin D per day
If you are in the sun a lot in summer, you can pause with vitamin D during this time. But probably no alarmingly high value would develop if you continued to take it despite sunbathing.
Correct intake: Always with a little fat
If you have vitamin D preparations that are available as powder in capsules if taken with black coffee, water or juice, this leads to absorption of the vitamin, but to a rather low absorption. As a fat-soluble vitamin, vitamin D should always be taken with a little fat. Like a glass of milk or Cholesterol lowering milk drinks or joghurt.
Too much fat is not a good idea either. So if you take the vitamin preparation with a thick lard bread or fatty cheese, you cannot take the ideal dose of it either. Because excessive amounts of fat seem to inhibit absorption.
A 2013 study found that taking vitamin D with 11 grams of fat resulted in absorption 16 percent higher than taking with 35 grams of fat and 20 percent higher absorption than taking with 0 grams of fat.
It doesn’t matter whether you get fat out polyunsaturated fatty acids (Hemp oil, Linseed oil, Sunflower oil), one made from monounsaturated fatty acids (olive oil, Avocados, Almonds) or one made of saturated (coconut oil).
Correct intake: Topical via the skin
If you cannot tolerate vitamin D preparations or whose vitamin D level simply does not want to rise despite the correct intake of vitamin D preparations, the vitamin can also be applied to the skin, since it can also be absorbed through the skin.
To do this, choose a liquid preparation without unfavourable additives, e.g. Vitamin D3 drops, which only come from vitamin D3 and MCT fats (medium-chain fats from e.g. Coconut oil) exist. Apply to the forearm, where the skin is particularly receptive
Important note
Disclaimer: This article was based on (at the time of publication) current studies written and checked by doctors, but may not be used for self-diagnosis or self-treatment, replaced so not to visit your doctor. So, discuss each one Measure (whether from this or another of our articles) always first with your doctor.
I hope you feel inspired. Look after your body, and it will keep you healthy.
By Dr Catherine W Dunne MSc. D., RGN, Reiki Master (RGMT), M.H.I.T: Master Acupressure, Practitioner of Reflexology, Aromatherapy, Deep Tissue/Myo-fascia Massages, Infrared Treatments, Vibrational Sound and Colour Therapist, Tissue Salt Advisor, Pendulum Healing Dowser, Chakra Practitioner , Tao Cosmic Healing Practitioner, Practitioner of Plant and Herb Medicine and Nurse.
Disclaimer: this article I have translated from German to English. In Germany and in USA, they are conducting research regarding best cholesterol lowering treatment, by focusing on Lipoprotein-a. Lipoprotein-a is the cause of fatty livers and the clogging up your coronary arteries. This research is still ongoing with very good outlook. The result is that we may only need a once per annum treatment. Sounds good to me, we’ll see.
Meanwhile, I stumbled across this German article and find it interesting enough to translate for you and share with you.
I hope you will enjoy the read.
Catherine.
Naturally lower Lipoprotein-a
Lipoprotein-a, a relative of cholesterol, is increasingly measured during medical examinations. The lipoprotein-a value is even more important than cholesterol levels when it comes to avoiding cardiovascular disease, they say. We explain how you can lower your lipoprotein-a naturally.
Lipoprotein-A – often abbreviated to Lp(a) – is mainly formed in the liver and consists of 2 proteins, apoliprotein A and apolipoprotein B. It belongs to the blood lipids and is related to LDL cholesterol.
Lp(a) is intended to contribute to the development of Arteriosclerosis and have a prothrombotic effect, which means that it promotes thrombosis (blood clots). Therefore, an Lp(a) value that is as healthy as possible would be ideal. There are hardly any drugs that lower the Lp(a) value. We explain how you can naturally lower your Lp(a) level and thus also reduce your cardiovascular risk.
How lipoprotein-a damages the vessels
Lp(a) damages the vessels and promotes arteriosclerosis as follows ( 1 ):
Promotes inflammation
Penetrates the arterial wall, thus enlarging the lesions (injuries) of the vessel walls, which aggravates atherosclerosis
Attaches more strongly to the blood vessel walls than LDL cholesterol
Interferes with the formation of plasmin, an enzyme that would dissolve blood clots
Lipoprotein levels: Which ones are good, which ones are bad?
Lipoprotein-A levels should not exceed 25 – 30 mg/dl (for us in Ireland and UK this translates to 0.06-0.08mmol/L. Another example: if your total cholesterol is 6.4 mmol/L this converts to: 247.5mg/dl). If you have higher values (they can rise to 400 mg/dl (10.3 mmol/L) and more), then you assume a massively increased risk of cardiovascular disease, namely for :
Aneurysm of the main aorta – An aneurysm is an abnormal bulge or ballooning in the wall of a blood vessel
Aortic valve calcification
Venous thromboembolism – Venous thromboembolism (VTE) is a condition that occurs when a blood clot forms in a vein. VTE includes deep vein thrombosis (DVT) and pulmonary embolism (PE). DVT occurs when a blood clot forms in a deep vein, usually in the lower leg, thigh, or pelvis.
With values above 120 mg/dl (3.1mmol/L), the risk is said to increase 3.6-fold.
Are high Lp(a) values genetically determined?
The personal Lp(a) value is considered to be genetically determined and can neither ne influenced on in any direction – neither upwards nor downwards. So even if the Lp(a) level is too high, it is said that this is “predisposition”. It can therefore hardly be reduced by a change in diet or other lifestyle changes (sports, stress management, weight loss).
Nevertheless, it is precisely these measures that are important even in the case of an elevated Lp(a) value. This is because the cardiovascular risk is particularly increased if there is at least one other risk factor.
So even if your Lp(a) value cannot be influenced, you should do everything you can to avoid any other risk factors (no smoking, no obesity, no diabetes, no high blood pressure, relatively good cholesterol levels, plenty of exercise, healthy eating, etc.). (1).
What factors can increase the Lp(a) value?
Even though Lp(a) levels are considered to be genetically determined, there are some factors that can increase Lp(a) levels – namely some conditions, such as Hypothyroidism (underactive thyroid), kidney disease and a Diabetes mellitus (Type 2 Diabetes(1).
If the Lp(a) level is now elevated due to such a disease, it can of course also be lowered if the causative disease can be alleviated. In the links above you will find measures that help with hypothyroidism and measures that help with diabetes (you may want to set your search engine to translate those pages for you).
Medications that lower Lp(a) levels
There are hardly any drugs that can lower the Lp(a) level and even if they do, they often do not lower the level low enough to reduce the cardiovascular risk. PCSK9 inhibitors (PCSK9 inhibitors are a type of cholesterol-lowering drug. They reduce your levels of low-density lipoprotein (LDL) cholesterol, or “bad” cholesterol.), for example, are used to lower cholesterol, but can also lower lipoprotein-a somewhat, but only by 30 to 40 percent.
PCSK9 inhibitors include the active ingredients alirocumab (Praluent), evolocumab (Repatha) and inclisiran (Leqvio), which are injected subcutaneously for 14 days or monthly. The drugs are very new (maximum approval in 2015), so that side effects are not yet fully known.
Pain and redness often occur at the injection site. However, it can also cause upper respiratory tract infections, itching (pruritus), headaches, joint pain, nausea, aching arms or legs, and fatigue.
The drug AKCEA-APO(a)-L Rx (pelacarsen), which also has to be injected – and in a placebo-controlled study achieved an 80 percent reduction in lipoprotein when administered 20 mg weekly ( 2 ).
Cardiovascular patients or high-risk patients are often given statins to reduce cholesterol levels. However, there are conflicting results on the effect of statins on lipoprotein levels. In two studies from 2016 and 2017, lipoprotein levels even increased at the beginning of statin therapy (1).
In any case, it is important that you know that lowering Lp(a) levels does not necessarily reduce cardiovascular risk (as there are simply too many risk factors for this).
So, you can’t say that we are now lowering the lipoprotein-a value by all means and are then protected from cardiovascular diseases. Therefore, we always point out a holistic approach and advise against always concentrating only on certain values that you now absolutely want to influence.
Lowering lipoprotein – natural remedies
A 2019 study looked at whether natural remedies or supplements known to lower LDL cholesterol levels could also affect lipoprotein levels (1):
L-Carnitine
Coenzyme Q10
Red Rice Yeast
Pectin
Ginkgo Biloba
Linseed
Curcumin
Coffee
Vitamin D
A number of remedies actually had a correspondingly positive effect. Nevertheless, the reduction was not so great for any of the preparations that – if a really high level was present – harmless values could be achieved. It is possible that a more significant reduction in the values could be achieved by combining several natural remedies, but this has not (yet) been investigated to our knowledge.
In the following studies, it is repeatedly recommended to combine the aforementioned remedies with blood lipid-lowering drugs, which should of course be discussed with the doctor.
L-carnitine is produced in the organism from the amino acids lysine and methionine. The substance is particularly involved in the production of energy from fatty acids (which is important for the adult heart, for example) and is therefore also referred to as a fat burner in some places. It is possible that L-carnitine can inhibit the formation of lipoprotein-a in the liver.
Coenzyme Q10
According to a meta-analysis from 2016, coenzyme Q10 can also reduce lipoprotein somewhat – by 12.5 to over 30 percent (by up to 11 mg/dl (0.3mmol/L)) when taking 120 to 300 mg daily over a period of 4 to 12 weeks. For the analysis, 6 studies with a total of 409 patients were examined. All patients suffered from lipid metabolism disorders.
Q10 doses of less than 150 mg were able to reduce Lp(a) levels more significantly than doses above 150 mg. The higher the original values, the better the patients responded to Q10. Other blood lipid levels, such as LDL cholesterol, HDL cholesterol or triglycerides, were not affected by Q10 intake.
Since Q10 is also used in naturopathic medicine against Side effects of statins if you have to take statins, you can also combine it very well with them and achieve a double goal (fewer side effects and a decreasing Lp(a) level).
In a randomized placebo-controlled trial from 2003, patients (with coronary artery disease) were given 1.2 g of red yeast rice per day for 6 weeks and experienced a 23 percent reduction in lipoprotein.
However, red yeast rice extract is not a blank slate, but basically contains nothing more than a natural statin (lovastatin) – and can therefore also have statin-like side effects. It is only less concentrated, therefore better tolerated, so it has a lower risk of side effects.
Statin-related side effects can be reduced by taking coenzyme Q10 – see the section on coenzyme Q10 – so if you want to try red yeast rice, it is best to take coenzyme Q10 as well.
Blood lipids are reduced by red yeast rice because it suppresses cholesterol formation – by inhibiting the so-called HMG‐CoA reductase. It is precisely through this mechanism of action that statins also act.
Pectin
Pectin is a soluble fiber that is abundant in apples or citrus peels. Because pectin has such good gelling abilities, it is also used to boil down jam.
As a dietary supplement, it has long been known to lower cholesterol – presumably because it promotes the breakdown of cholesterol in the liver, but also because it could inhibit the absorption of cholesterol and bile acids in the intestine. (If bile acid is not absorbed in the intestine, but is drained out with the stool, then the liver produces new bile acid from cholesterol, which then naturally leads to a decrease in cholesterol).
A study from 1999 examined whether pectin could also lower lipoprotein-a. In the placebo-controlled, double-blind study, patients (who suffered from high blood lipid levels) received 15 g of pectin daily (for 4 weeks), after which the level of lipoprotein decreased by up to 27 percent.
Ginkgo Biloba
Extracts from the leaves of Ginkgo biloba are usually used for dizziness, tinnitus or for Alzheimer’s prevention. The main effect of the plant is to promote blood circulation. However, it also has anti-inflammatory, antioxidant and antiatherosclerotic properties. Antiatherosclerotic means counteracting vascular calcification.
In a first clinical study in 2006, for example, the administration of 120 mg of extract twice a day after 2 months was able to reduce lipoprotein by 23.4 percent or an average of 10.4 mg/dl (0.3mmol/L) – presumably due to the inhibitory effect on numerous pro-inflammatory messenger substances (cytokines).
In a 2007 study, ginkgo was even able to reduce atherosclerotic deposits in the blood vessels after 2 months in patients who were to receive a bypass. The same dose was used here as in the 2006 study – in the form of the special ginkgo extract EGb 761®, which is contained in numerous ready-to-use ginkgo preparations ( 4 ).
Linseed
Since fiber is generally considered to lower blood lipids and cholesterol, it should generally be part of a healthy diet for lipid metabolism disorders or an increased cardiovascular risk. Linseed consists of almost a quarter (23 percent) of fiber and is therefore particularly suitable here.
In addition, flaxseed contains certain plant substances with high health potential for the cardiovascular system, such as omega-3 fatty acids (cholesterol-lowering) and Lignans (blood lipid-lowering, antioxidant, anti-cancer in breast cancer and prostate cancer).
In a double-blind crossover study with postmenopausal women from 1998, however, flaxseed showed only a small reduction in lipoprotein levels. After six weeks of taking 38 g of flaxseed daily, the value had fallen by 7.4 percent and by an average of just under 2 mg/dl (0.1mmol/L) (1).
From 2008 comes another study (randomized, controlled, double-blind) in which the subjects were asked to eat 40 g of flaxseed per day for 10 weeks. The lipoprotein value decreased by an average of 14 percent compared to a group of patients who took wheat bran (1).
The reduction in the Lp(a) value is therefore rather small, but combined with the other positive effects of flaxseed on cardiovascular risk, it is quite relevant. For example, the small seeds have been able to slow down the progression of arteriosclerosis in various studies (1).
Curcumin
As curcumin, the active ingredient complex is used in Turmeric denoted. It has a positive effect on triglycerides and cholesterol levels, but also on lipoprotein levels. A 2014 randomized controlled trial found that taking 1g per day (for 8 weeks) increased lipoprotein levels in people with Metabolic Syndrome (Metabolic syndrome is a group of conditions that together raise your risk of coronary heart disease, diabetes, stroke, and other serious health problems.) by almost 10 percent (8 mg/dl (0.2 mmol/L)).
Curcumin has anti-inflammatory and antioxidant properties, among other things, and can also reduce cardiovascular risk and support health through these mechanisms of action.
Coffee
Coffee consumption also influences blood lipid levels – due to at least two active ingredients: kahweol and cafestol. However, the content of these two substances in coffee depends on the method of preparation.
If the coffee is made with a paper filter, the active ingredients are apparently largely removed from the drink, so that it has no influence on cholesterol levels. Coffee prepared without filters, on the other hand, could increase LDL cholesterol levels.
In connection with lipoprotein-a, it seems that short-term coffee consumption reduced plasma lipoprotein levels, while regular coffee consumption is associated with higher levels.
Ginger
In a 2020 study, patients with atherosclerosis took capsules containing 1.6 g of ginger powder daily or capsules containing a placebo. After 8 weeks, two values that are elevated in atherosclerosis had dropped significantly – the value of lipoprotein-a and the hs-CRP value (an inflammatory marker that indicates the condition of the blood vessels and helps to assess the risk of heart attack) ( 5 ). In the 2019 paper (1), it was still said that ginger could not lower lipoprotein-a, which does not seem to be true in every case, so ginger can be very well integrated into an Lp(a)-lowering diet plan.
With Lp(a) ≧ 30mg/dl and vitamin D < 10 ng/ml, the risk of coronary heart disease increased more than 4-fold
The risk was 1.79 times higher for Lp(a) < 30mg/dl and vitamin D < 10 ng/ml
The risk was 1.7 timeshigher with Lp(a) ≧ 30mg/dl and vitamin D ≧ 10 ng/ml
In each case compared with patients who had an Lp(a) of less than 30mg/dl and a vitamin D level of more than 10 ng/ml.
The study thus shows that a higher vitamin D level can significantly reduce the cardiovascular risk with a high Lp(a) value! Read all about the correct dosage and Taking vitamin D.
This is also an example of the fact that naturopathic measures may not always be able to lower the lipoprotein level (or not strongly enough), but the cardiovascular risk associated with an increased lipoprotein level can be reduced.
These substances cannot lower lipoprotein
Some natural substances lower LDL cholesterol levels, but not – according to various studies – lipoprotein (1), e.g.
Berberine
Brazil nut flour
Garlic
Olive oil
Onions
Vitamin C
Soy protein and soy isoflavones
Of course, you can still incorporate these foods into your diet or – in the case of vitamin C – take them as a dietary supplement. After all, these are generally very healthy foods that have many beneficial properties and – even if they cannot specifically lower lipoprotein-a – still reduce the cardiovascular risk, and that’s what matters in the end.
Important note
This article was written on the basis of (at the time of publication) of current studies and reviewed by medical professionals, but may not be used for self-diagnosis or self-treatment, so it does not replace a visit to your doctor. Therefore, always discuss any measure (whether from this or another of our articles) with your doctor first.